Constrictive Pericarditis
Patients with constrictive pericarditis are usually chronically ill and present with signs and symptoms of increased right and left heart filling pressures such as fatigue, dyspnea, ascites and pedal edema. Some patients present with a chief complaint of increased abdominal girth. A history of prior episodes of pericarditis or conditions associated with pericardial involvement such as cancer, chest trauma, tuberculosis or prior cardiac surgery is uncommon.
The appearance of patients with constrictive pericarditis may be so dramatic, that it can occasionally lead to a false diagnosis of cirrhosis of the liver.
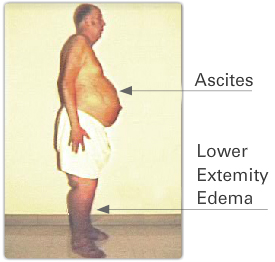
The patient shown here has marked ascites, a common physical finding of constrictive pericarditis. He also has severe lower extremity edema due to markedly elevated central venous pressure from the constriction.
On physical examination, patients with constrictive pericarditis show increased central venous pressure along with prominent "x" and "y" descents. In some, Kussmaul's sign is present that is, a rise in central venous pressure with inspiration. This is due to the inability of the right heart to accept an inspiratory increase in right ventricular volume without a marked increase in filling pressure. An enlarged liver and a pericardial knock may also be present. Pulsus paradoxus occurs, although less frequently than with cardiac tamponade.
A pericardial knock is a diastolic filling sound that is higher in frequency and earlier than a typical third heart sound. It reflects the sudden deceleration of blood entering primarily the right ventricle due to a stiff restrictive pericardium. It is best heard at the left sternal edge and is frequently louder during inspiration.